If we have one mission, it is to remove complexity from the delivery of behavioral health and IDD services. The right workflows and insights:
Streamline care processes
Automate tasks to reduce staff burdens
Provide clinicians more time to deliver quality care
You’ll see how providers are using Core to reach new levels of clinical and financial performance while freeing up staff’s time and energy for what matters most: client care.
Who Uses Core?
Our EHR is specially designed to meet the unique needs of practice managers and clinicians working in behavioral health, substance use, IDD and child & family services practices.
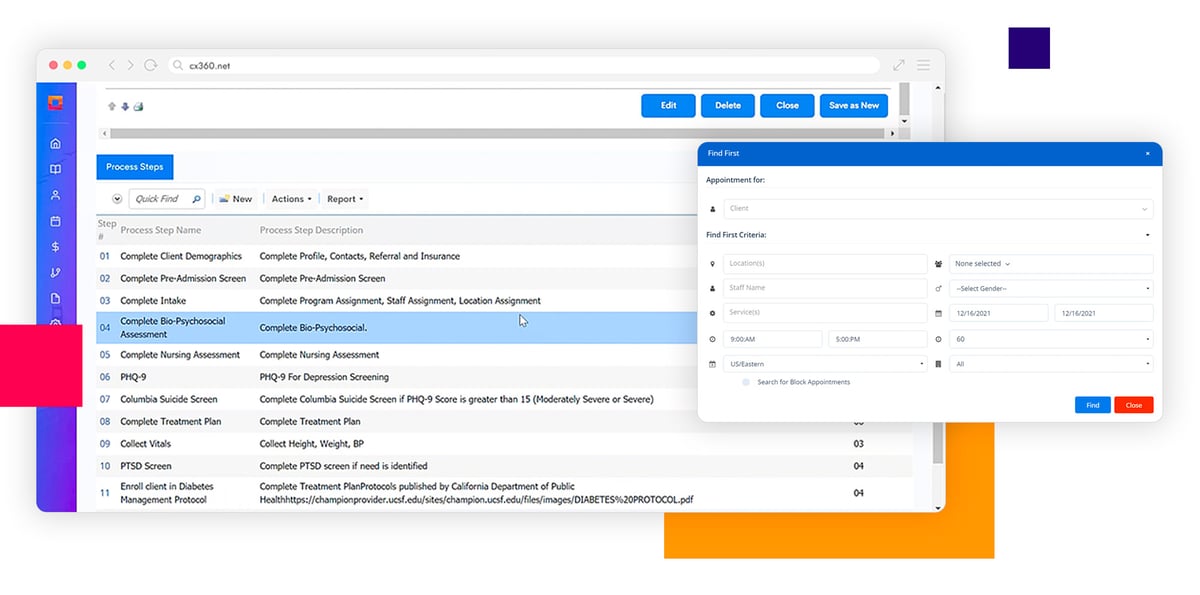
Improve Quality of Care
Enable clinicians and other staff to get the most out of their time and efforts with intuitive tools, automations, seamless telehealth and customizable workflows.
Optimize Billing & Collections
Make fewer errors and collect more for your practice’s hard work with smart, easily scalable billing tools and automated patient follow-up that take the complexity out of the financial parts of care.
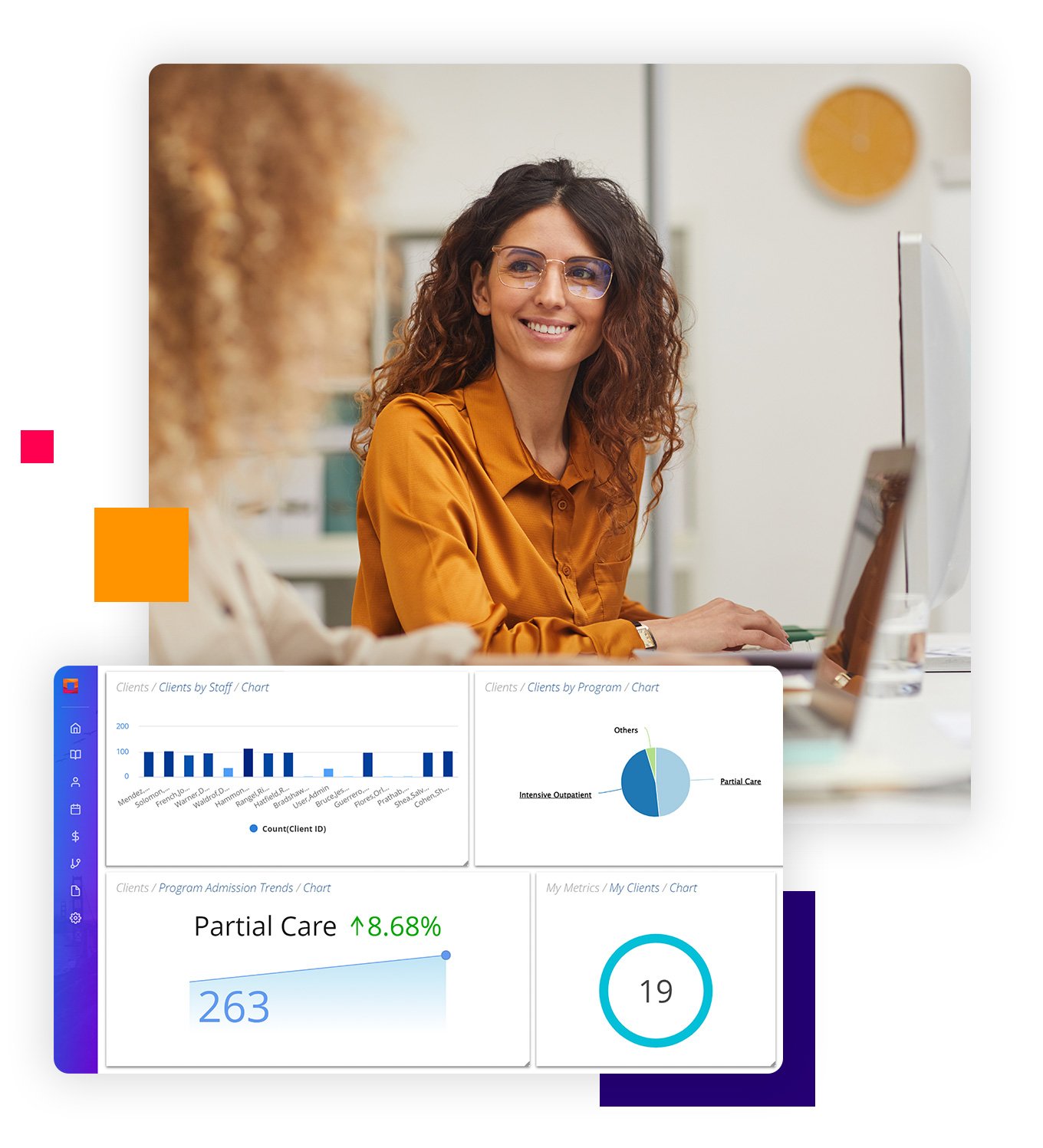
Get One View – the Right One
With new levels of clinical and business insights, you’ll be able to identify best practices and pursue the types of strategies that drive meaningful—and measurable—success.